Disorders of the thyroid are a common cause of swelling in the neck and are typically asymptomatic. When they do cause symptoms, it tends to be
related to the mass or goiter pressing on the airway or esophagus resulting in the feeling of something pressing in with resulting difficulty
breathing or feeling like food or liquids get caught on swallowing. Masses of the thyroid are usually discovered by the primary care doctor.
After a short workup which typically includes an ultrasound to better characterize whether there is one nodule or multiple. Thorough research
in thyroid masses has been compiled by the American Thyroid Association into an evidence based set of
guidelines on when masses should be biopsied and what sort of treatments should be undertaken thereafter, or even if any are required.
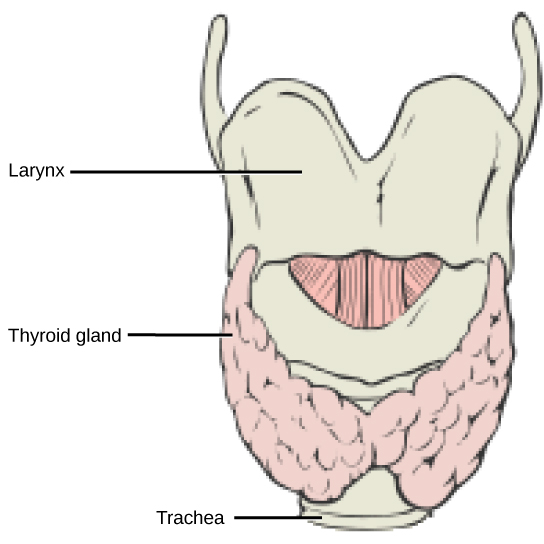
Image by CNX OpenStax [CC BY 4.0], via Wikimedia Commons
Typically, masses will be biopsied when they reach a certain size and feature criteria. This biopsy will usually come back in one of three general
categories. The first category is that the nodule is suspicious for or diagnostic of a cancer which requires further workup including imaging of
the neck, either by ultrasound of the sides of the neck, or CT scan with contrast. In times past, contrasted CT scans were avoided as there was
fear that it would delay possible radioactive iodine treatment if it was needed; however modern research shows this is not usually longer than
6-8 weeks which is indeed not a significant delay. If the nodule is contained solely within the thyroid based on imaging, typically either a
thyroid lobectomy (taking out half of the thyroid) or a total thyroidectomy is the only prescribed treatment. One of the more exciting developments in Thyroid cancer research
is the increasing evidence that tumors less than 4cm in greatest dimension without aggressive features may be simply treated with thyroid lobectomy
rather than a total thyroidectomy. The benefit of this less aggressive surgery is that thyroid hormone replacement usually is not required post-
operatively. Additionally, some of the more serious complications that are remotely possible with a total thyroidectomy are not possible with
only a thyroid lobectomy. Not all tumors are able to be treated in this conservative manner, and a unified treatment decision with the patient,
endocrinologist, and thyroid surgeon is of paramount importance when this conservative manner is chosen as the tumor surveillance (making sure
the cancer isn't coming back) is somewhat more complicated.
Fortunately, the majority of thyroid biopsies will return benign in which case conservative observation is the usual management recommendation.
Occasionally, the patient may rather proceed with elective thyroid lobectomy rather than continuing to conservatively observe. This is
particularly true if the nodule or goiter is causing symptoms such as trouble swallowing or feeling of something impeding breathing. Surgical
removal is also typically chosen if the nodule or goiter is visible under the skin.
Occasionally, the biopsy sample will come back in a category that is uncertain. This is the typical case when the cells visualized are felt
to be follicular cells or Hurthle cells. Historically, every patient in this category would have required surgery to check whether or not cancer
was present. This is because the only way to diagnose cancer with this particular cell type is to evaluate the wrapper surrounding the nodule. If
follicular cells were found to be crossing through and going out of this wrapper, it was diagnosed as a follicular or Hurthle-cell cancer.
However, with the advent of modern molecular testing, 60-70% of patients in this category are able to be further reclassified as "likely benign"
and thus avoid surgery! This should always be discussed with your thyroid surgeon or endocrinologist because even if your insurance refuses to
pay for it, many times it can be done on a cash basis for around $300.
If you have been diagnosed with a thyroid nodule, or told that you need surgery for a thyroid disorder, make an appointment with Dr York today,
CLICK HERE!
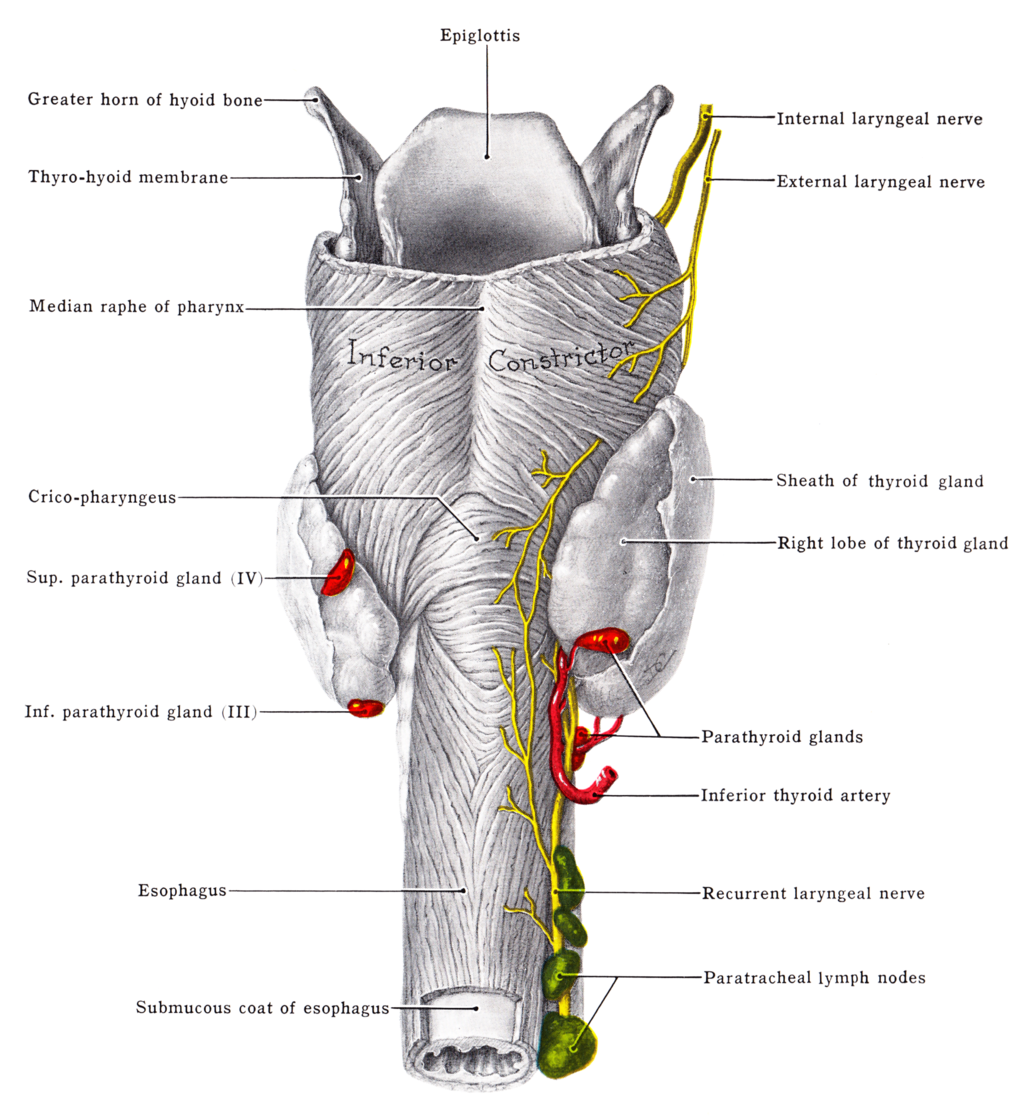
Parathyroid Disorders
Image by Grant, John Charles Boileau (An atlas of anatomy, / by regions 1962) [Public domain], via Wikimedia Commons
The most comon parathyroid disorder is a single parathyroid adenoma. Patients with a hyperfunctioning parathyroid adenoma will frequently complain
of fatigue, mood disorders, kidney stones, or stomach ulcers. These are typically diagnosed on routine labwork which shows an elevated calcium
level. This is due to increased parathyroid hormone which causes the bones to release extra calcium. Other disorders can cause increased
parathyroid function such as some congenital endocrine disorders (such as multiple endocrine neoplasia syndromes). The typical treatment for
parathyroid hyperfunction is removal of the single adenoma or mass causing it. If it is due to increased size of all 4 parathyroid glands, removal
of 3 and a half glands is recommended. Rarely, scanning will identify what is felt to be a single adenoma; however on surgery, the parathyroid
hormone level doesn't go down sufficiently requiring removal of the other 2 and a half glands.
If you have been diagnosed with a parathyroid nodule, or hyperparathyroidism, make an appointment with Dr York today,
CLICK HERE!

{kind=link}
{kind=link}
{kind=link}